![]()
REGULATIONS FOR EXAMINATION OF HEART AND BLOOD VESSELS IN THE US ARMY, 1917
The following was taken from the Landry Papers and details the medical examination of the cardio-vascular system required for recruits for the US Army in 1917.
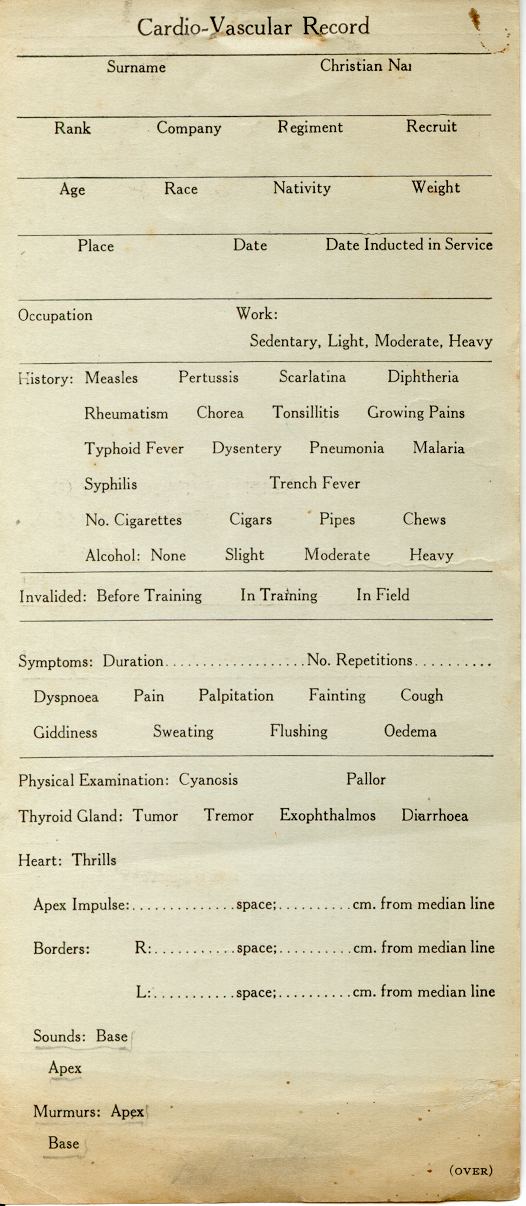
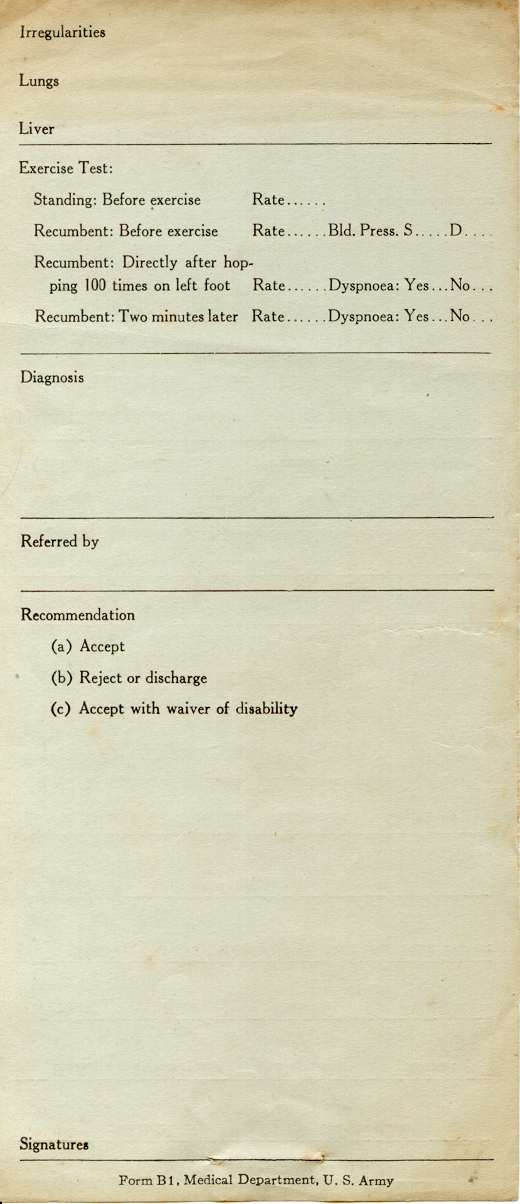
Cardio-Vascular record card, front and back, Form B1, Medical Department, US Army
The examination should include in all cases,-
(a) Location and determination of character of apex impulse.
(b) Auscultation of the heart sounds over apex, lower sternum, and the second and third interspaces to right and left of sternum, noting accentuation of sounds and murmurs.
(c) Inspection of root of neck and upper part of thorax and percussion of first interspace on each, side of manubrium for evidence of aneurysm.
(d) Count of radial pulse, observation of its rhythm and palpation of radial arteries for unusual thickening of high tension.
(e) Exercise test; Hopping 100 times on one foot. At close count heart rate with stethoscope over apex, listening for murmurs and noting how long tachycardia and unusual dyspnea persist, After two minutes neither should be marked.
Note;
(1). Apex if outside nipple line, or below fifth interspaces.
(2) Any murmurs.
(3). Signs or symptoms of Aneurysm
(4) Radial pulse- if
a. Rate over 100
b. Irregular
c. Arteries markedly thickened.
d. Pressure increased
If any of above noted do hopping test and take blood pressure. (e)
REJECT ALL MEN;
(1) With signs of circulatory failure, ie. breathlessness, cyanosis and oedema,
(2). With apex outside nipple line or in 6th interspace, Determine cause.
(3). With murmurs and conditions as in (2).
(4). With aneurysm.
(5) with constant pulse rate of 100 or more, with demonstrable cause, or over 110 -without cause.
(6).With blood pressure of 160 systolic or 100 diastolic.
(7). With signs of erythromelalgia or Raynaud's disease.
(8) Who give a history of thrombo-phlebitis and show swelling and loss of function.
DEFER ALL MEN;
(1) With murmurs transmitted in classical directions showing no cardiac hypertrophy.
(2) Those having a constant pulse rate between 90 and 100 without demonstrable cause,
(3) With pulse of 50 or under.
4) With thrombo-phlebitis of upper extremities.
HEART MURMURS. ( McKenzie.)
FUNCTIONAL MURMURS,
(1) Systolic,
(2) Tricuspid or mitral orifice,
(3) Soft and blowing,
A rough murmur, accompanied by a purring tremor or musical note indicates valve lesion.
MITRAL STENOSIS;
(a) Presystolic murmur over a small area around apex, terminates in the first sound; crescendo character; presystolic thrill.
(b) Mid-diastolic murmur.
(c) Diastolic murmur, diminuendo in character.
MITRAL INSUFFICIENCY.
Systolic murmur, loudest at apex, may be soft or blowing, not transmitted, or rough and loud, transmitted over whole heart area, axilla and back. A rough, loud murmur with thrill indicates damaged valve.
AORTIC STENOSIS,
Systolic murmur loudest over 2nd right costal cartilage and propagated into the carotids. It may be faint or prolonged with a thrill over upper part of chest wall. Heart slow; pulse impinges against finger in a slow leisurely fashion
AORTIC INSUFFICIENCY,
Diastolic murmur, somewhat long drawn out, sometimes very brief; propagated down the sternum, and sometime heard loudest at apex.
This murmur is usually associated with aortic stenosis, giving the characteristic double -aortic (bellows) murmur,- Galloping (Corrigan's Water Hammer) pulse.
Systolic Murmurs Accidental, Insignificant;
(a) These heard at Apex on excitement, especially when recumbent;
(b.) Those heard over 2nd and 3rd left interspace dung expiration, disappearing during forced inspiration.
(c) Systolic accentuation of the respiratory murmur, especially on inspiration, heard near apex or over the back;
(d) Other Systolic murmurs unassociated with enlargement of the heart, alteration of the first sound, accentuation of the pulmonic second, or abnormal responce to exercise may also be considered without significance but should be noted.
(e) Loud Systolic murmurs, audible at the apex, and in the left back, if associated with any enlargement of the heart, with snapping first sound, or accentuated pulmonic second, will be cause for rejection. If unassociated with these other signs and response to exercise be normal, accept for limited service.
Systolic murmurs at the base, heard in the 2nd right intercostal space, harsh, conveyed well into the neck, associated with Aortic Diastolic murmur, with thrill, or with marked enfeeblement of Aortic second sound, shall disqualify.
Accept - Slight Systolic murmurs in this situation, with no other abnormal sign, and response to exercise.
Diastolic Murmurs;- All Diastolic murmurs at apex or at neck, reject, including presystolic murmurs. Look for enlargement of one or both sides of the heart, alteration of the 1st or 2nd sound, particularly snapping first sound and accentuated pulmonic second in Mitral disease and the characteristic pulse of Aortic Insufficiency.
Aneurysms of the Thoracic Aorta;
Pulsation above the base of the heart, diastolic shock, well marked dullness laterally to the manubrium with a ringing second sound or a systolic or diastolic murmur over the dull area, or tracheal tug, inequality of the pupils, difference in the two radial pulses, alteration of the voice, are suspicious signs of Aneurysm.
(Form 64, pp 50-56)
Return to Landry Papers Index
Return to Medical Front Index