
THE TECHNIQUES OF BLOOD TRANSFUSION
The
earlier operators, owing to the difficulties introduced by the
coagulation of blood outside the body, were constrained to make use of
some method of direct transfusion, the blood flowing directly from an
artery of the donor into the patient's veins. This has now been largely
replaced by one of the methods of indirect transfusion, the blood being
withdrawn from the donor into a vessel in which clotting is delayed or
prevented, and then injected or allowed to run into the patient's
circulation.
Direct Transfusion.
- The obvious method of performing a direct transfusion is by making an
end-to-end anastomosis between an artery of the donor and a vein of the
recipient. The most readily accessible artery is the radial at the
wrist, and this is indeed almost the only artery that is available. The
most accessible vein is the median basilic or the median cephalic at
the elbow. The operation of end-to-end anastomosis, using an artery of
so small a calibre as the radial artery at the wrist is usually found
to be, is one of great technical difficulty ; this effectually
prevented transfusion from being used at all frequently. A modification
has been used by Sauerbruch and others, in which the end of the radial
artery is drawn into the lumen of the vein through a slit in its wall.
A suture is passed through the radial artery close to its cut end, and
the needle is then passed through the slit in the vein and out again
through the wall of the vein an inch or so higher up. Traction on the
suture then pulls the artery into the vein. The artery has meanwhile
been temporarily occluded by a clip, which is removed when the artery
is inside the vein, so that the blood can then flow from one to the
other. This is easier to do than the anastomosis, but, in addition to
the other objections to direct transfusion to be mentioned presently,
the difficulty occurs of occlusion of the artery by the physiological
process of inversion of its coats at the cut end. This is likely to
happen before much blood has passed, so that apparent success at first
is often not maintained. Sauerbruch claimed that the amount of blood
that had passed could be estimated by measuring the time taken for 1
cc. of blood to flow from the artery before it was introduced into the
vein ; but there is no proof that the rate of flow remains constant.
If direct transfusion be desired, there can be no doubt that Crile's
method, introduced some fifteen years ago, is the best to employ. After
much patient work Crile perfected a method of anastomosis which ensures
that no occlusion of the vessels can take place at the site of
junction. This depends on the use of a short silver tube, through which
the end, of the artery is threaded. The artery is then pulled back
again outside the tube in the form of a cuff and fixed in position. The
end of the artery has thus been made rigid, and over this the vein is
pulled in its turn and fixed by a ligature. A watertight junction is
thus made, and blood can flow through it without interruption unless
clotting takes place in the vessels as the result of handling and
injury to their walls. This method has been extensively used in
America, and it was the first to render the operation of transfusion a
comparatively popular one.
Various other devices for achieving the same result have been
elaborated by other workers, and attention may be drawn to those of
Elsberg and Bernheim, both of which are described in the book by the
latter on " Blood Transfusion." During the war a simpler method was
introduced by Colonel Andrew Fullerton, who, working at a Base Hospital
in France, found that he could get good results by employing a thin
rubber tube with a small silver cannula at either end. The apparatus
was first coated on the inside with a thin layer of paraffin wax, in
order to discourage clotting within the tube, and the cannula were
introduced into the donor's artery and the recipient's vein
respectively. The blood could then flow freely from one to the other.
The fact that blood was being transmitted was taken to be proved by the
visible pulsation of the thin rubber connecting-tube synchronously with
the arterial pulsations. The disappearance of this was assumed to be
evidence that clotting had occurred. This method was described by
Colonel Fullerton to the surgeons working at the Casualty Clearing
Stations, where blood transfusion was likely to be of most service, but
it was never used extensively. The coating of the inside of the tube
with paraffin is in itself an operation of some difficulty. Under
conditions in which any loss of time could not be permitted, success by
this method was not attained with sufficient certainty, and it, was
shortly afterwards replaced by the more satisfactory methods described
below. The most recent work on direct transfusion has been done by J.
M. Graham at Edinburgh, who has however reached the conclusion that
the. technique is always more difficult than that of indirect
transfusion.
It can easily be seen, therefore, that all the known methods of direct
blood transfusion present great technical difficulty, which renders the
method unsuitable for general use. There are, in addition, certain
other objections to it of an obvious nature. It is, in the first place,
impossible to measure the amount of blood which has passed from the
donor to the recipient. Sometimes an indication may be obtained from
the evident improvement in the condition of the patient, acconipanied
by the signs of loss of blood in the donor. More often clotting takes
place, unknown to the operator, at some point, with the result that
blood ceases to pass a considerable time before the end of the
operation, and the patient has consequently received very much less
blood than is supposed. It has been claimed by Libman and Ottenberg
that the amount of blood transferred may be estimated by weighing the
donor before and after the operation. This presupposes that a very
accurate weighing machine is easily available, which usually is not the
case.
A second objection is the extent of the injury which is necessarily
inflicted on the donor. His radial artery must be exposed through an
incision of considerable length, and must be ligatured at the
conclusion of the process. The operation becomes, therefore, a matter
of some moment to the donor, who will be permanently scarred, and can
under no circumstances be used for transfusion more than twice.
A third objection is that the transfusion cannot be done with due
regard to the condition of the patient. A delicate and difficult
operation has to be performed with the donor and recipient lying side
by side, their arms close together. It is therefore almost
imperative that both should be on operating-tables of a convenient
height. Often, however, with an exsanguinated patient it
is important that he should not be moved from his bed, but as a bedside
operation direct transfusion becomes difficult indeed!
A final objection is that in some people the, radial artery is of very
small calibre, so that when all preparations have been made, and the
artery exposed, it is found to be quite impossible to proceed. Another
element of uncertainty is thus introduced.
There is, therefore, little to be said in favour of direct transfusion,
and much to be urged against it. This method has, indeed, in my own
opinion, come to be of historical interest only. For this reason the
different methods have only been very briefly described.
Indirect Transfusion.
- The methods of indirect transfusion may be divided into those which
depend upon the use of an anticoagulant mixed with the blood and those
in which the blood is given unaltered. The technique of either process
is simple compared with that of direct transfusion, though any method
which makes use of whole blood can never be quite as free from
uncertainty or difficulty as one which introduces the use of an
anticoagulant. If the blood is prevented from clotting, the chief cause
of failure in performing blood transfusions is removed. With any
whole-blood method of transfusion speed is exceedingly important,
frequent practice is a very great advantage, and it is essential, as
with direct transfusion, that the donor and recipient should be in
close proximity to one another, if not actually side by side.
On the other hand, the use of an anticoagulant renders speed and
frequent practice of less account. The blood can be drawn, and can then
be put on one side until the best moment for giving it has arrived. Due
regard may be had to the patient's condition, since the blood can be
carried about and can be given at leisure to the patient in his bed
without disturbing him and almost without his knowing it. The donor,
too, is not exposed to the mental shock of lying for some time side by
side with a patient who may be in extremis, or may even expire during
the operation.
There are, however, those who consider that the use of whole blood,
instead of blood which has been chemically treated, has advantages
which outweigh the possible disadvantages mentioned above. Two methods
of using whole blood are, therefore, described first; the use of
anticoagulants is then described in detail, and their advantages and
possible dangers are enlarged upon.
Whole Blood Transfusion with Syringes.-
It is obvious that, if blood can be drawn from the donor's vein into a
glass syringe and injected into the recipient so rapidly that clotting
has no time to occur, then a transfusion of any quantity of blood that
may be wished can be given by this simple means. The measure of the
amount of blood transfused is given by the number of syringes that have
been filled and emptied. This method has been successfully used by
several workers, and it has the adVantage that no very gpecial
apparatus is necessary. It does, however, require that several
syringes, and more than one assistant, should be available since
clotting will take place in the syringes, unless they be frequently
washed out. There is also the possibility that clotting may take place
in the needle which is introduced into the donor's vein, since this
cannot be withdrawn and replaced for each syringeful of blood that is
transferred. With practice, however, and with good assistants, the
process can be done quickly enough to avoid this. Wide-bore needles
with short rubber connexions are introduced into the veins of donor and
recipient ; if, as often happens, this is difficult to do through the
skin in the case of the recipient, his vein must first be exposed
through an incision and a glass or metal cannula introduced into it.
The operator then fills the syringes with blood in quick succession and
hands them to his first assistant, who injects the blood into the
recipient. Blood is prevented from escaping from the needles when the
syringes are disconnected by nipping the rubber connnections with the
fingers. The first assistant passes the empty syringes to the second
assistant, who washes them out with normal saline, and hands them back
if needed to the operator. This can be done with six 20 cc. syringes
used in rotation, possibly with only four.
The most recent description of this method has been published by J. M.
Graham of Edinburgh, who has introduced an improved form of needle.
This consists of a double tube; the inner tube has a needle point which
is used for puncturing the vein, and can be withdrawn into the blunt
outer tube when the vein has been entered. Any further wounding of the
vein is thus avoided. In addition, movement of the needle-cannula is
prevented by a bull-dog forceps attachment, which is clipped to the
skin. Graham finds it advisable to lubricate the cannula and syringes
with vaseline before being used. He also states that: "As the absence
of clotting depends upon the rapidity with which the syringes are
filled and emptied, a series of syringes should be used in strict
rotation, and all trace of blood must be washed out with saline before
the syringes are used again. One or two additional assistants are
necessary for this method." The disadvanta ges are evident, and it is
not suitable for general use.
A modification of the method has been described by Unger, in which only
one syringe is used. The barrel of this is cooled by an ether spray so
that clotting is discouraged or prevented.
Whole Blood Transfusion with Kimpton's Tube.-The
principle of this method depends upon the use of paraffin wax as a
coating for the vessel into which the blood is drawn, so that clotting
is prevented or greatly delayed. The form of the vessel has been
modified by different workers, but the essentials are the same in each.
One form of the apparatus, known as the Kimpton-Brown tube, consists of
a graduated glass cylinder, of about 700 cc. capacity, the lower end of
which is drawn out into a cannula point at an acute angle with the body
of the cylinder; the point is of a size convenient for introducing into
a vein and its bore large enough to allow of a free flow of blood
through it. Near the upper end is a side tube to which a rubber tube
can be attached, and an opening at the top is closed by a rubber hung.
An ordinary rubber double-bulb bellows is the only other apparatus that
is needed.
The glass vessel is first sterilized in the autoclave, and then it must be coated on the inside with a thin layer of paraffin wax. The whole success of this method depends upon this wax coating being absolutely complete right up to the tip of the cannula at the bottom. If the tiniest area of glass be left exposed in the cannula, the process will fail. The production of this perfect wax coating used to be exceedingly difficult of attainment without very frequent practice. The apparatus was first raised to exactly the right temperature; sterile, melted paraffin was then put into it, and distributed evenly over the surface, excess being allowed to run out. The apparatus was then cooled down, and could be put away in a sterile towel ready for use, great care being taken that the lumen of the cannula was patent and not blocked with excess of wax. A simplification of the process was introduced by the use of a saturated solution of wax in ether. This solution is put into the vessel, which must not be heated, and is made to run all over the surface, excess as before being allowed to escape through the lower opening. The. ether quickly evaporates, leaving a very thin and perfect film of wax over the surface of the glass. As before, it must be ascertained that the lumen of the cannula is patent. The apparatus is then ready for use.
The
donor and recipient need not be lying close together, but they must be
in the same room. A vein is exposed in the arm of each by dissection
under.a local anaesthetic. The operator then picks up the vein with a
pair of dissecting forceps, and makes an oblique cut into the lumen. A
flap is thus made which is held in the dissecting forceps in the left
hand or is picked up with a fine-pointed pair of artery forceps, The
Kimpton's tube is taken in the right hand, and the point of the cannula
is introduced into the vein ; that part of the lumen lying opposite the
flap serves as a gutter which guides the cannula directly into the
lumen, so that it is introduced without any fumbling or delay, The
cannula. is pushed on so that its widest part engages the whole
circumference of the vein, forming a joint through which blood does not
leak. The cannula having been pushed well up into the vein, the forceps
holding the venous flap may be let go. At the same time air assistant
grips the donor's upper arm, or some form of tourniquet of the
necessary degree of tightness is applied, so that the veins become
congested without obliteration of the arterial pulse. Blood now flows
rapidly into the tube, and the venous pressure is always sufficient to
overcome the counter-pressure of the increasing head of fluid in the
tube. It is unnecessary, therefore, to produce any negative pressure
within the tube with a reversed Higginson's syringe or an exhaustion
pump, which has been used by some workers. Blood is allowed to flow
into the tube until the requisite amount has been obtained. The venous
congestion is then released, and at the same time the tube and cannula,
held at the lower end with the right hand in such manner that the index
finger is free, is withdrawn from the vein. At the moment of withdrawal
the end of the cannula is closed with the right index finger. To
prevent haemorrhage from the donor's vein, a ligature previously put
round it is tied by an assistant, or pressure on it is maintained with
a sterile swab. The operator must now, without a moment's delay, carry
the tube filled with blood over to the recipient. An opening in his
vein is made by an assistant in the same manner as already described,
the finger is removed from the cannula, and its point is instantly
introduced into the vein. It is now necessary to produce some degree of
positive pressure in the tube to ensure that the blood shall at once
begin to flow steadily into the vein. This is done with a rubber
bellows, attached by an assistant to the upper side tube, and the level
of the blood in the tube should at once begin to fall. Great care must
be taken that the positive pressure is released before the tube is
completely emptied of blood in order to avoid the obvious danger of the
entry of air into the patient's vein. When the tube is nearly empty it
is withdrawn, the vein is ligatured, and the wounds in donor and
recipient are sutured. The most convenient pattern of Kimpton-Brown
tube holds only about 500 cc. of blood, so that if more is needed, the
process must be repeated.
There is virtually only one cause of failure in transfusion by this
method, and that is the occurrence of clotting in the cannula or at the
bottom of the tube. If it does occur at any stage of the operation, it
cannot be remedied. It may happen when the tube is nearly full; if so,
the blood that has been withdrawn cannot be used. Clotting may be due
to an imperfection in the paraffin coating on the glass, but if there
is any delay from any cause, it may take place independently of this.
The method is therefore never absolutely certain of success even in the
hands of an expert, and for general use it is certainly unsuitable. It
was introduced into the British Army by some of the American surgeons
in 1917, and was used by the writer under the guidance of Major Alton
of the Harvard Medical Unit during the first battle of Cambrai with
good results. Many of the English surgeons, however, soon abandoned it
as a routine method in favour of anticoagulants. There are other
objections to it besides its uncertainty. A vein must be exposed by
dissection in both donor and recipient, so that avoidable injury is
inflicted on the former. It is not a perfectly clean method, some blood
necessarily escaping at each successive stage in the process, though an
expert can reduce this to a minimum. In the hands of a novice it may
occasion a very bloody scene. The whole operation is one of urgency,
and the best interests of donor and recipient cannot always be
considered.
Modifications have been introduced, such as that of Vincent, who uses an attachment with a needle instead of the glass cannula point. This obviates some of the objections, but introduces other difficulties, such as the necessity for coating the inside of the needle with paraffin wax. The technique can certainly be acquired, and the method has rendered excellent service in the past, but it has no obvious advantages except the uncertain one of avoiding chemical treatment of the blood.
Transfusion with Anticoagulants.-
It will have become evident from the descriptions of the transfusion of
whole blood already given, how great a difficulty is introduced into
the technique of these methods by the physiological process of clotting
in blood outside the body. It is clear how much the process of
transfusion would be simplified if the clotting were to be prevented.
Something has already been said in the historical sketch of the various
means by which this problem was attacked, and it need only be stated
here that the most suitable substance for this purpose has been found
to be sodium citrate. This method was introduced by Lewisohn as
recently as 1915, and It soon became the method of choice among most of
those who tried it.
The process of the formation of a blood clot has always been one of the
great problems of physiology, and numerous theories have been
propounded to explain it. The theory accepted at the present time
regards the process as a complicated one depending on the presence in
the blood of a number of different factors. This theoretical
explanation may be represented diagramatically as follows:
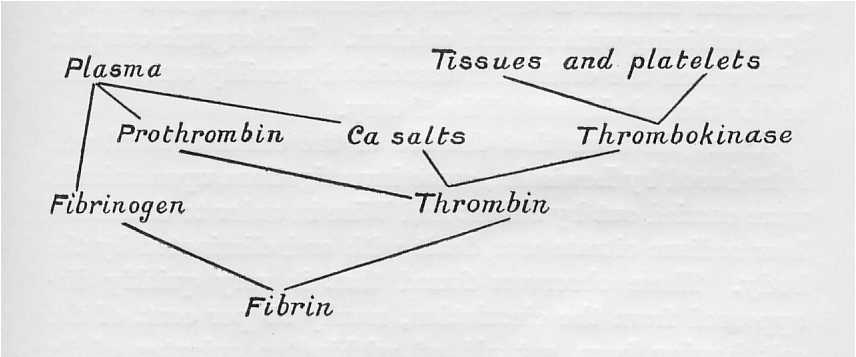
The
clot consists of fibrin in which blood corpuscles are entangled. It is
clear that if any one of the reacting agents can be removed or rendered
inert the clotting cannot take place. There is only one inorganic
substance taking part in the reaction, and it is this factor that is
more easily removed than any of the others. Calcium is precipitated in
an insoluble form by various chemical reagents, but it is obvious that
for purposes of transfusion the formation of an insoluble precipitate
is not permissible. It is therefore necessary to use a substance which
will form a soluble compound with the calcium and which is at the same
time harmless when introduced into the circulation. The only substance
which has been found at present to possess both these properties is
citrate of sodium. This forms with calcium a soluble double salt, in
which calcium is rendered inert. It is usually held that the calcium to
be active must be present in the ionized form, but recent
investigations by Vines into the role of calcium tend to modify
slightly the accepted view of its action. He has shown that calcium is
present in the blood in two forms, ionized and combined, and that both
take part in the coagulation reaction. He has, in addition,
demonstrated that a quantity of anticoagulant sufficient to combine
with the whole of the calcium present in a given quantity of blood is
not enough to prevent coagulation. It seems, therefore, that the
anticoagulant acts by combining with a large organic molecule of which
calcium is only one constituent, and not merely by combining with
ionized calcium. The organic complex with which the calcium is
associated possibly corresponds to the thrombokinase of the theory.
About the time that the use of the citrated blood was introduced by
Lewisohn, some investigations upon animals were carried out
by Salant and Wise in order to determine how sodium citrate was
dealt with and eliminated by the body. These observers found that it
very quickly disappeared from the circulation, nearly 90 per cent. of
the salt having been got rid of within ten minutes of its intravenous
injection. Part of the citrate is destroyed by oxidation, and the rest,
30 to 40 per cent., is eliminated by the kidneys, the urine being
rendered alkaline. It was also shown that if a very large dose was
given, so large that toxic symptoms resulted, the effect was rapidly
obtained; but that if the toxic dose were not fatal, no remote effects
followed. Its injection never rtsulted in any albuminuria.
Lewisohn showed by experiment on the human subject that up to 5 grammes
of sodium citrate in the form of a 0.2 per cent. solution could be
injected intravenously with the calcium and which is at the same
time harmless when introduced into the circulation. The only substance
which has been found at present to possess both these properties is
citrate of sodium. This forms with calcium a soluble double salt, in
which calcium is rendered inert. It is usually held that the calcium to
be active must be present in the ionized form, but recent
investigations by Vines into the ro1e of calcium tend to modify
slightly the accepted view of its action. He has shown that calcium is
present in the blood in two forms, ionized and combined, and that both
take part in the coagulation reaction. He has, in addition,
demonstrated that a quantity of anticoagulant sufficient to combine
with the whole of the calcium present in a given quantity of blood is
not enough to prevent coagulation. It seems, therefore, that the
anticoagulant acts by combining with a large organic molecule of which
calcium is only one constituent, and not merely by combining with
ionized calcium. The organic complex with which the calcium is
associated possibly corresponds to the thrombokinase of the theory.
About the time that the use of the citrated blood was introduced by
Lewisohn, some investigations upon animals were carried out by Salant
and Wise in order to determine how sodium citrate was dealt with and
eliminated by the body. These observers found that it very quickly
disappeared from the circulation, nearly 90 per cent of the salt having
been got rid of within ten minutes of its intravenous injection. Part
of the citrate is destroyed by oxidation, and the rest, 30 to 40 per
cent, is eliminated by the kidneys, the urine being rendered alkaline.
It was also shown that if a very large dose was given, so large that
toxic symptoms resulted, the effect was rapidly obtained; but that if
the toxic dose were not fatal, no remote effects followed. Its
injection never resulted in any albuminuria.
Lewisohn showed by experiment on the human subject that up to 5 grammes
of sodium citrate in the form of a 0.2 per cent. solution could be
injected intravenously with out any harmful results. It was also shown
that this concentration of the salt was sufficient to prevent clotting
outside the body, and that the microscopic appearance of the blood
cells was not altered by the admixture of this solution.
Theoretically, therefore, the amount of citrate that should be used as
an anticoagulant should be 2 grammes for 1,000 cc. of blood, or 100 cc.
of 2 per cent. solution for 900 cc. of blood. In practice it is better
to err on the side of safety and to use a slight excess of citrate.
This amount of citrate should be used for the 750 cc. of blood which
constitutes the ordinary maximum amount of blood used in a transfusion.
For smaller quantities of blood the amount of citrate may be
correspondingly reduced.
The use of citrated blood was introduced to the British Army in France
in 1917 by Oswald Robertson, who recommended the use of a larger amount
of citrate than this. His object in increasing the amount was to
produce a solution which, when diluted with the correct amount of
blood, would be isotonic with it. It was thought that a hypotonic
solution might result in some damage to the red corpuscles by osmosis,
and Robertson therefore recommended the use of 160 cc. of a 3.8 per
cent. solution of citrate, which, when mixed with 750 cc. of blood,
will give a solution of which the osmotic pressure equals that of 0.9
per cent. saline solution. It may be doubted, however, whether this
consideration is of more than theoretical importance. There can be
little doubt that in practice the effect of a slightly hypotonic
solution, such as is given by the solution of citrate, is negligible as
regards destruction of corpuscles. If, however, it be thought
necessary, an isotonic solution may be produced by the addition of
sodium chloride. Other considerations, as will be seen shortly, weigh
in favour of giving the smaller amount of citrate. The dosage to be
recommended, therefore, on practical and experimental grounds is 2
grammes of citrate, in 100 cc. of water for 900 cc. of blood, or 1
gramme of citrate in 50 cc. of water for 450 cc. of blood or less.
These proportions need not be observed very accurately. Latitude may be
used in either direction without harming either the transfused blood or
the patient.
It has been stated above that sodium citrate introduced into the
circulation in small quantities, such as are sufficient for
anticoagulant purposes, is non-toxic to man. In the light, however, of
the extended experience of the last four years, it is seen to be
possible that this statement may not be quite literally true. Probably
there is an individual variation in the tolerance of different people
to sodium citrate. Certainly in some cases a reaction follows the
injection of citrated blood. The symptoms of this reaction are a slight
headache, a rise in temperature to two or three degrees above normal,
sometimes accompanied by a rigor or a sensation of chill, and an
increase in the pulse rate. The effect is, however, always very
transitory, lasting only two or three hours, and is never, in my own
experience, attended by any symptoms which need give rise to anxiety
for the patient's welfare; nor does it in any way prejudice the
therapeutic results of the transfusion.
That
the reaction is caused by the citrate and not by another constituent of
the transfused blood has been believed by several observers. In a case
seen by the writer a slight citrate reaction occurred in a youth who
acted as blood donor. The transfusion was carried out by a modification
of the syringe method, which involved the injection at intervals of a
syringeful of citrate solution into the donor's circulation. The
possibility that the reaction was produced by another factor was
therefore not present in this instance.
Nevertheless, it must be admitted that citrate has not yet been
absolutely proved to be the cause of this slight reaction in all the
cases in which it occurs. Evidence has, indeed, been brought forward by
Lewisohn and by Meleney to show that citrate is definitely not
responsible for the reaction. The statement is made that some reaction
occurs after 10 per cent. of all transfusions, and that this percentage
is unaffected whether whole blood or citrated blood is used. Lewisohn
has himself investigated the effects in a long series of parallel cases
in which different methods were employed, and he reports that the
results following the use of citrated blood were as good as with any
other method. Drinker states that reactions follow the use of citrated
blood slightly more often than they do that of whole blood, but this
has not been confirmed. He was unable to find any impurity in the
citrate that might be held responsible. It is quite possible that all
the reactions observed are in reality caused by the " minor agglutinins
" mentioned on p. 73. Meleney has noticed that the blood of some donors
is more likely to produce a reaction than that of others ; this
suggests that the responsibility rests with the blood and not with the
citrate. The occurrence of a toxic reaction constitutes the only real
objection to the use of citrated blood that has yet been brought
forward, but even this has not yet been fully substantiated ; in any
case, the reaction is of so little importance that it is greatly
outweighed by the numerous advantages that are conferred by the use of
citrate. The possibility that a citrate reaction does sometimes occur
may be taken as an indication in favour of using the smaller amount
recommended by Lewisohn rather than the larger dose used by Robertson.
The experience of a great many observers has established the fact that
citrated blood is quite as effective as whole blood in its therapeutic
effects.
It is convenient to have the sodium citrate in a form ready for
immediate use. I have therefore been in the habit of keeping it in the
solid form in small stoppered bottles, each containing 1 gramme of the
salt. These are sterilized at 130 degrees C, and can be kept
indefinitely until wanted. If 450 cc. of blood or less are to be drawn,
the contents of one bottle is shaken into the transfusion flask; 50 cc,
(approximately 2 oz.) of sterile warm water are added, in which the
citrate will rapidly dissolve. If more than 450 cc. of blood is to be
used, the contents of two bottles must be dissolved in 100 cc. or 4
ozs. of water. Alternatively a concentrated solution of citrate may be
kept in scaled ampoules. but the salt is less stable in solution, and I
prefer to keep it in the solid form.
The ideal method of blood transfusion seems to me to require that it
shall be absolutely certain of success, that the blood shall not
necessarily be injected into the patient immediately it has been drawn,
so that other circumstances besides the demands of the transfusion
operation can be considered, and that no injury shall be done to the
donor beyond the puncturing of a vein. In addition to this, the method
should be so simple and free from special apparatus that it can be
easily learnt and carried out by one operator without skilled
assistance. All these require. ments are fulfilled by the citrate
method, and a satisfactory method of performing this will next be
described. As will be seen, the blood can be drawn with the minimum
amount of injury to the donor; when drawn, it can be put on one side,
for several hours if necessary, and then given to the patient at
whatever may be judged to be the most favour. able moment the whole
process can be carried out by a single operator without any assistance;
and finally, but little practice is needed to make success certain
every time.
The
transfusion apparatus known as "Robertson's bottle," first described by
Oswald Robertson in 1918, is the basis of most citrate methods. This
could be easily improvised in a field laboratory, and was extensively
used during the last year of the war. The apparatus consisted of a
glass bottle of about a litre capacity, the mouth of which was closed
by a rubber bung. Through the bung three glass tubes passed. One,
connected by a short rubber tube with a wide-bore needle, ended about
an inch from the bottom of the bottle; through this the blood flowed
into the bottle. A second tube, which reached to the angle between the
side and the bottom of the bottle, was connected by a rubber tube with
a cannula; through this the blood was injected into the patient. The
third tube reached only just beyond the bung, and to this was attached
a Higginson's syringe, by means of which either negative or positive
pressure would be produced inside the bottle, according to which end of
the syringe was attached.
It is unnecessary to describe this apparatus any further, for it was
found by myself and others that it could be with advantage modified in
the direction of simplicity. It is in the first place unnecessary in
drawing the blood to create any negative pressure if a needle of a
large enough bore (2 or 3 mm.) be used, and, further, it is an
advantage not to have the needle attached in any way to the bottle,
which, as the blood flows into it, has to be freely agitated in order
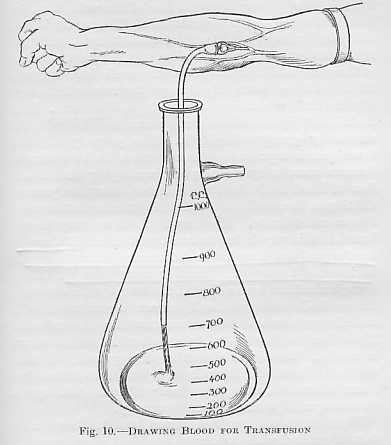
to mix the blood quickly with the citrate. The needle may, therefore,
be attached to a rubber tube of suitable length which hangs freely into
the collecting vessel as shown in the diagram:
The third tube of "Robertson's bottle" may be dispensed with by using a conical flask provided with a side tube to which a rubber bellows can be attached. The delivery tube is therefore the only one that need pass through the rubber bung. This tube should have. an angle in it inside the flask so that its lower end reaches into the corner, and the extremity should be ground down obliquely so that, although it reaches right into the corner, it does not become occluded by too accurate contact with the surface of the vessel. By this means any wastage of blood is prevented. I have found it a very great convenience to introduce into the delivery tube just outside the flask an air-lock, (This embodies the same principle as the "dropper" designed by R.D. Laurie) the value of which will he seen shortly. To the barrel of this air-lock a rubber tube with a cannula is attached. Close to ihe cannula is some form of clip. The. whole apparatus is illustrated in the figure, and with the help of this its use may be readily understood.
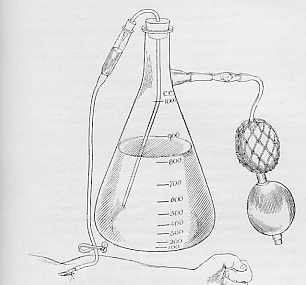
Injection of blood, showing use of airlock.
The particular form of needle which I have been in the habit of using is shown below.
![]()
Transfusion Needle
Its
lumen has a diameter of 2 mm., and the steel tube ends off flush with
the wide shoulder to which the rubber tube is attached. This avoids any
recess within the needle in which clotting may begin. The point of the
needle should not be too long, in order that it may not wound the
opposite side of the vein when it has been introduced. For ease of
introduction, however, the extremity should be very sharp and should
have cutting edges. The point and edges should be touched up on a
bevelled hone each time before the needle is used. The needle should be
kept ready for immediate use in liquid paraffin. I have found that the
most convenient way of keeping it is to put it into a test-tube
containing paraffin, which is plugged with cotton-wool and sterilized
at 130 degrees C. in the hot air oven or by careful heating over a
flame. In this way the needle may be kept ready for an indefinite time
without any chance of its rusting. When it is taken out of the
test-tube, a sterile rubber tube is slipped on to it and it is then
ready for use. As an additional precaution, a small quantity of
paraffin may be drawn up into the rubber tube, which is thus lubricated
on the inside, but this is not absolutely necessary. The tube must be
sterilized with the rest of the apparatus, as rubber is destroyed by
liquid paraffin.
When the donor's arm has been congested by gripping it above the elbow,
or better by the application of a tourniquet drawn to the requisite
degree of tightness, a suitable vein, usually the median basilic, is
chosen. The area of puncture is washed with ether and a very small
quantity, 2 to 8 minims, of 2 per cent. novocain is introduced over the
vein with a hypodermic syringe. If a larger quantity is used, the vein
may become obscured, but this small amount may be dispersed by a few
moments' pressure with the finger, and is usually enough to anxsthetize
the very small area of skin that is to be operated upon. A tiny cut in
the skin is then made with the point of a scalpel, and the needle is
pushed through into the vein. If the donor's vein is a large one, such
as is usually found in the type of donor recommended in a previous
chapter, this is quite easy to do. To make it equally easy if the vein
be smaller, it has been suggested by Watson that the vein may be fixed
by pushing an ordinary fine sewing-needle through the skin at right
angles to the line of the vein, into the vein, and out again through
the skin. This needle is held with the forefinger and thumb of the left
hand, while the right hand pushes the transfusion needle into the lumen
of the vein just below it. When the needle is in the vein, the blood
flows out rapidly through the tube which hangs into the flask
containing the citrate, as illustrated. This flask is held by an
assistant, who mixes the blood with the citrate by gently swinging it.
If a properly adjusted tourniquet is kept on the donor's arm while he
works his forearm muscles by clasping and unclasping his hand, a flow
of blood is obtained which is fast enough to prevent clotting in the
needle, and indeed is quite as fast as most donors can tolerate. Blood
up to 1,000 cc. may be collected in this way in ten to twenty minutes.
If the vein be of a good size, it makes no difference whether the
needle be insertedtowards the heart or away from it. When enough blood
has been collected, the tourniquet is removed, the needle is withdrawn,
and pressure is maintained with a sterile swab over the site of
puncture for a few minutes. No further bleeding will take place after
this, and no suture is needed. The donor's part in the operation is
then finished. He should be made to lie on his back for a few hours
afterwards, and given plenty of fluids, but beyond this no special.
precautions are necessary.
When the blood has been drawn, and has been satisfactorily mixed with
the citrate, the flask may be put on one side until it is wanted, its
mouth having.been closed with a cotton-wool stopper. If the blood is
wanted at once, the flask may be stood in a basin of warm water to keep
it at body temperature. Otherwise it may be allowed to cool, and can be
warmed up again when it is to be administered. The citrated blood may
be kept for a considerable time without undergoing any appreciable
change in its therapeutic value. It has been given twelve hours or more
after being taken with the same good effects as if it had been newly
drawn. During the war advantage was taken of this fact to anticipate
during quiet times the necessity for many transfusions during times of
stress. The blood was drawn in some quantity and kept for several hours
in an ice chest, so that it was readily available during the expected
battle. Recently I have administered to a woman who had been operated
upon for a ruptured ectopic gestation 600 cc. of citrated blood which
had been kept for twenty-seven hours at room temperature after it was
drawn. The effect was in every way as satisfactory as if it had been
freshly drawn, and there was no sign of any toxic reaction. So far as I
know, blood had not ever been kept so long as this before being used,
but there does not seem to be any objection to so doing.
When the blood is to be given, the delivery tube with the rubber bung
is inserted in the flask, and the corpuscles which have gravitated to
the bottom are distributed again. through the fluid by gently shaking
it. In administering the blood, it is very often advisable to inject it
through a cannula which is tied into a vein. If the patient is a woman,
it will usually be found that the veins are small and buried in fat.
Also many transfusions will be given to combat the collapse due to
shock and haemorrhage, in which case the veins will be empty and the
use of a cannula will be found essential. Sometimes, however, the
patient will have large veins which can be readily distended; this may
sometimes be encouraged by keeping the arm for half an hour beforehand
in a bath of hot water. Under these circumstances the blood can be
given through a needle introduced in exactly the same way as has
already been described in the case of the donor. In the following
account of the process it will be assumed that the use of a cannula is
necessary.
When choosing a vein in the patient,the operator must be guided
by,circumstances, Usually the median basilic will be the most
convenient, and if, in a collapsed patient, this is invisible, previous
knowledge of the position of the vein mustdetermine the site of the
incision. If another operation is being done simultaneously upon the
upper part of the patient's body, it may be more convenient to use the
internal saphenous vein in Searpa's triangle, or even one of the
superficial veins about the ankle.
Whatever vein be chosen, the line of the incision is first infiltrated
with a small quantity of a 2 per cent. solution of novocain. The vein
is then dissected out, and is ligatured near the lower end of the
incision. A ligature is also put loosely round the upper part. The
operator now takes the barrel of the air-lock, which, together with the
attached rubber tube and cannula, is filled with 0.9 per cent. saline
solution, all air bubbles being carefully excluded. The. tube is
clipped near the cannula, so that the whole system, including the
cannula, remains filled with the fluid. The form of the cannula used
will depend upon the operator's particular preference, but a type which
I have found very convenient is shown in the accompanying figure. It is
made of glass, and its extremity is ground down at an angle, which
makes it very easy to introduce into the vein. The slight constriction
near this end ensures that it can be securely tied into the vein and
that no leakage round it shall occur. This is very necessary,
because there is sometimes a considerable pressure to be overcome, due
to venospasm in a collapsed patient, before the blood, begins to flow.
![]()
TRANSFUSION CANNULA
An oblique cut is now made in the vein, as shown in the illustration, the cannula is introduced, and the upper ligature is tied.
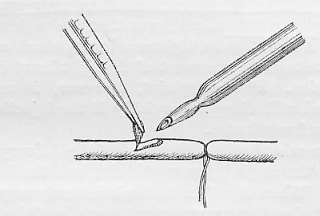
INSERTION OF CANNULA IN VEIN
The barrel of the air-lock, with its contained saline solution, is then fixed firmly on to the rubber bung, so that the nozzle of the delivery tube projects into the saline solution. Meanwhile, an assistant has fixed a rubber bellows on to the side tube of the flask; a short piece of glass tubing loosely packed with cotton-wool should be interposed between the bellows and the flask to prevent any particles of dust being blown over into the flask from the bellows, which is not sterilized, The clip near the cannula is released, and some positive pressure is produced inside the flask by means of the bellows. The citrated blood then rises in the delivery tube, and a corresponding quantity of saline solution is displaced from the air-lock into the patient's circulation. The blood then flows from the nozzle of the delivery tube into the air-lock, and the remainder of the saline solution is driven on into the patient. Finally the blood flows steadily through the cannula, and the rate at which it is flowing can be observed in the air-lock.
The
presence of this air-lock facilitates, as has been seen, the
introduction of the cannula into, the vein since there is no leakage of
blood to obscure the operation. In addition,
the operator can see at a glance whether the blood is flowing in
properly, and can regulate the rate of flow to a nicety by varying the
pressure in the flask by means of the bellows. If a very slow injection
is required, the blood can even be. made to run drop by drop. If the
patient is suffering from acute anaemia, the blood can be pumped in
rapidly, 750 cc. of blood being given in the course of twenty minutes.
If, on the other hand, the patient has a plethora of fluids, such as is
seen in some cases of secondary anaemia, the blood must be given very
much more slowly than this, since it is dangerous rapidly to increase
the blood volume. A half to three-quarters of an hour must be occupied
in giving 500 cc., and even then the patient may complain of a
sensation of tightness in the chest and of dyspncea, due to
embarrassment of the right heart during the transfusion. This
complaint, however, is usually transient, and will disappear quickly if
the injection be stopped for a few minutes.
It has been said that the lower end of the delivery tube reaches into
the angle between the side and the bottom of the flask. When therefore
the flask is nearly empty, it should be tilted so that very nearly the
whole of the blood can be forced up the tube. When the flask is quite
empty, the blood in the barrel of the air-lock must be carefully
watched, and when its level has fallen to the bottom of this, the clip
must be applied to the tube above the cannula. By this means no
blood is wasted except the small quantity which remains in the tube
below the air-lock. As soon as the tube has been clipped the cannula is
withdrawn, the vein is ligatured above the opening into its lumen, and
the edges of the skin incision are sutured.
Transfusions carried out in this way can be performed with uniform
success. The technique is simple and straightforward at every stage,
and can be easily demonstrated and learnt. It is, in addition, a
perfectly clean process, and not a single drop of blood need be spilt.
Any method which involves the injection of blood under pressure is open
to the objection that it is possible to over-look the fact that the
flask has been emptied and to kill the patient by injecting air into
his veins. This can, however, only happen as the result of great
carelessness on the part of the operator. The presence of the air-lock
affords an additional safeguard, as it can hardly escape the operator's
notice that blood has ceased to flow from the nozzle of the delivery
tube.
The method may also be criticized on the ground that some damage is
caused to, the corpuscles of the donor's blood by the shaking which is
necessary to mix it with the citrate solution. This objection is, in my
opinion, theoretical rather than practical. If, however, it be desired
to avoid any such shaking, the apparatus designed by A. E. Stansfeld
and described by him in 1918 may be used. This ensures that the citrate
and the blood flow into the containing vessel together, so that no
further mixing is needed. The apparatus is more cumbrous, more fragile,
and less easy to clean and to sterilize than that described above. In
the hands of an expert it will give excellent results, but its use
requires some little practice, and it is therefore not so well adapted
for general use.
The whole of my own apparatus, as described above, may be obtained from
Messrs. Allen & Hanburys, Wigmore Street, London, W.1, who also
provide a convenient box for carrying it.